|
 |
|
|
|
|
|
Jules Gonin. Pioneer of Retinal Detachment
Surgery
Thomas J Wolfensberger, MD, PD, MER
Development of the Ignipuncture
The promotion to chairman of the Eye Hospital and to
the professorship gave Gonin a new burst of energy to
continue his research. Between 1919 and 1934 he published
40 papers which all dealt either with the pathogenesis
of retinal detachment, or with the surgical treatment
and its results.4,5 The key
papers were read at the annual meetings of the Swiss,
French or German Ophthalmological Societies. Gonin had
realised, that the hole in the retina was not a consequence
of the retinal detachment, but that it was in fact the
origin of the detachment (Figure 4).
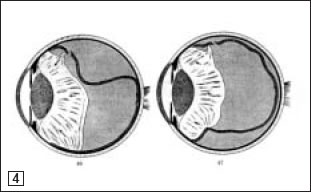
Figure 4. Drawing by Jules Gonin
explaining the tractional forces on the retinal break
induced by the posterior vitreous. (Drawing taken from
J. Gonin:"Le décollement de rétine"1934,
Payot, Lausanne)
He also rightly concluded that the retinal detachment
could only be treated if the retinal break was closed.
To this end he developed the therapy that would become
his trademark: the ignipuncture (Figure 5).
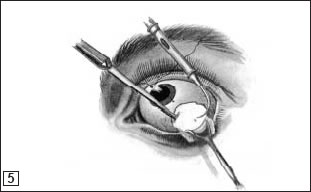
Figure 5. Illustration of the ignipuncture
procedure. After having localised the break and incised
the conjunctiva in that area, the surgeon pierces the
sclera with the Graefe knife and then applies the curved
thermocauter, which had been heated white, to the retinal
break through the small sclerotomy. (Drawing taken from
J. Gonin:"Le décollement de rétine"1934,
Payot, Lausanne)
This treatment consisted of localising the retinal break
with direct ophthalmoscopy. Gonin then ordered bedrest
with both eyes patched in a position favourable to the
resorption of subretinal fluid. As soon as repeated
examination showed that the subretinal fluid had resolved,
Gonin estimated in disc diameters the distance from
the tear to the ora serrata and converted it into milimeters
of distance from the limbus. After having incised the
conjunctiva in that area, he marked the site of the
break on the sclera. He injected novocaine into the
subconjuntival space, pierced the sclera with the Graefe
knife and then applied the curved thermocauter, which
had been brought to white heat, to the retinal break
through the small sclerotomy. At that time subretinal
fluid drainage often occured. The cauterisation induced
a chorioretinal scar where it was applied and help to
closure of the retinal break (Figures 6a & 6b).
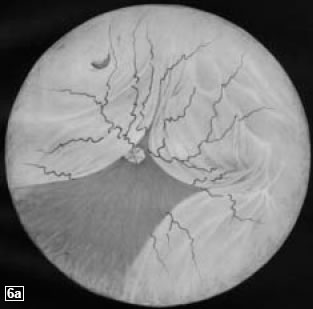
Figure 6a. Drawing of retinal detachment
in a left eye with a single break in the superonasal
quadrant (Drawing taken from J. Gonin:"Le décollement
de rétine"1934, Payot, Lausanne)
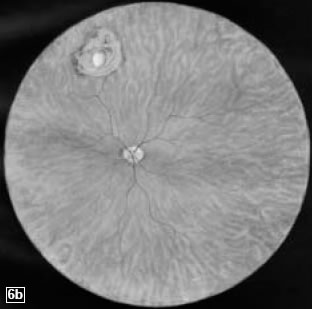
Figure 6b. The same eye after ignipuncture.
The retina is completely attached and a chorioretinal
scar is present around the retinal break. (Drawing taken
from J. Gonin:"Le décollement de rétine"1934,
Payot, Lausanne)
The conjunctiva was then sutured. The patient was subsequently
returned to bed with binocluar patching, and the head
was put in such a position that the retinal break was
at the lowest point allowing further subretinal fluid
absorption. Patients were usually bed-bound in this
strict position for at least a week.
In 1913 Gonin managed for the first time to treat a
traumatic retinal detachment using the procedure with
ignipuncture,6 and in 1916,
he repeats the same feat in an idiopathic retinal detachment.
In 1923 Gonin began to speak about his results at ophthalmic
meetings.7 With his new cure
he could increase the success rate from 1% to 30-40%.
Despite his clear results his colleagues were sceptical.
"You have not convinced anyone" was
the reaction of Professor Gabriel Sourdille, another
eminent retinal surgeon, whose technique to operate
retinal detachments was to make deliberate holes in
the sclera and the retina followed by the instillation
of weak mercuric cyanide solution around the sclerotomy
sites.1 It was not until
1929 that he received worldwide recognition at the International
Ophthalmological Congress in Amsterdam for his surgical
technique. Recognition from his home country came with
the Benoît Prize, the highest scientific honour
in Switzerland.
Jules Gonin's ideas of clinic management were that his
associates should enjoy complete freedom in how to run
their day-to-day clinical and surgical duties. The only
obligation of his associates was to lend him their patients
for his lectures. Thus the management of cataract patients,
as an example was very different. It depended purely
under which associates the patient was admitted to hospital.
Dr. Dufour preferred to do a sector iridectomy weeks
before the cataract extraction, Jules Gonin preferred
an extracapsular extraction with the iridectomy in the
same sitting and Dr. Amsler preferred intracapsular
extraction! Only the retinal detachment patients underwent
the same surgical procedure by Gonin himself. He had
no alphabetical file of his 38,000 patients but he would
even get indignant if one of his patients forgot his
code number from one visit to another1
(Figure 7a & 7b).

Figure 7a. Photograph of Jules
Gonin taken by de Jongh in the 1920s. (From: “Asile
des Aveugles: La pérennité d’une
vocation” Lausanne, 1993)
Figure 7b. Drawing of Jules Gonin
by a colleague in Lausanne in later years. (From:"Asile
des Aveugles" Lausanne, 1985)
Although the clinical duties at the hospital commanded
his wholehearted attention, Jules Gonin also found time
to spend with his family. He was a very keen observer
of the political scene in Switzerland.
When proportional representation in the government was
discussed, he and his father were strong supporters
of it. He also advocated the vote for women as well
as weighted votes; two votes for parents, and people
with high school certificates, and non-commissioned
officers, and three votes for parents of large families,
officers or university graduates.1
Other personal pursuits included the study of
the Arabic language and the collection of butterflies,
an interest which never left him after his initial research
on the metamorphosis of Lepidoptera during medical school.
Gonin also loved to travel. Once he was taken for a spy
in Greece and arrested. In Switzerland he travelled extensively
on foot, and also loved mountain climbing, particularly
if the path involved the crossing of glaciers.
|
|
|
|
|
| |

 History
History